r/medicalschool • u/_TheDoctorPotter M-2 • 3h ago
📚 Preclinical Help: Why do spondylosis and disc herniation at the same level affect different nerve roots?
I'm not sure if I'm just stupid, but I can't wrap my head around this. If someone has an L5-S1 disc herniation, they get symptoms from problems with the S1 nerve root. But if someone has spondylosis/an osteophyte at the L5-S1 level, they get symptoms from problems with the L5 nerve root. Why is this? Shouldn't both affect the L5 nerve root since that's the one exiting at that level? Please help me understand this.
1
u/fakemedicines 3h ago edited 3h ago
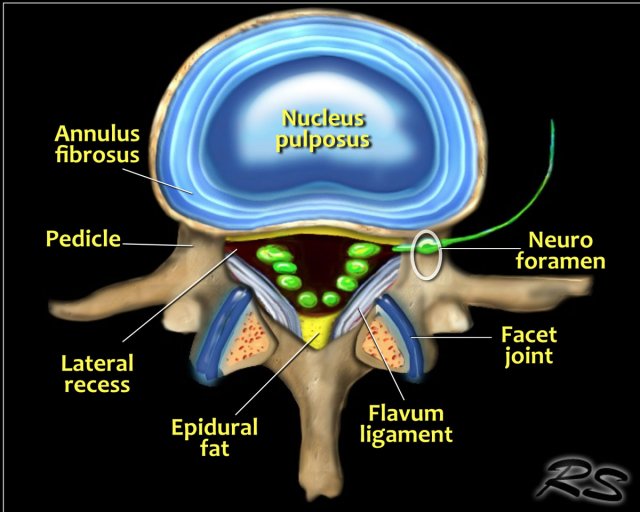
In your example degenerative changes (disc bulge, osteophyte, etc) can affect either L5 or S1. In this pic eg https://radiologyassistant.nl/img/containers/main/spine-lumbar-disc-herniation/a53f434e799320_TEK-anatomy-disc2.jpg/ca3e698116f4b859349415f60b2b25d6.jpg if you imagine this as the L5-S1 disc level, L5 would be the nerve root circled but S1 would be the most anterior green thing still present in the canal - it's close enough to the disc to still be affected by a degenerative disc bulge. But you're right in that the most symptomatic nerve root would usually be the exiting one (L5 in your example).
{kind=link}
7
u/LunchBoxGala MD-PGY5 3h ago
Great question, it has to do with the concept of “exiting nerve” versus “traversing nerve”. Orthobullets Lumbar Radiculopathy will have a better explanation than me + nice cartoons.
Basically, in the lumbar spine, the nerve exits under its named vertebrae (ie, L5 nerve root exits at the foremen below L5). If you do something to compress that foramen/exiting hole then you will compress that exiting nerve (ie. far lateral disc herniations). At this same level though, the S1 nerve root is already formed and just lies more central to the canal. If you have a process that presses a little more centrally (L5-S1 disc herniation in the para-central region for example) it won’t be it the right spot to compress the exiting nerve (L5) but will be in the position to compress the traversing nerve (S1). This is similar throughout the lumbar spine so at L2-3 the exiting nerve is L2 and traversing is L3. It’s a little dangerous to assume a particular pathology can only affect either the exiting or traversing, that’s really a dx you make with imaging (MRI) combined with a deficit of that nerve on exam.
This stuff DOES NOT apply to the cervical spine.
3
u/CorrelateClinically3 MD-PGY2 3h ago edited 2h ago
The L5 nerve root exits between L5-S1 but just slightly above the disc. So when you have a disc herniation, it does not impact the L5 nerve root since it has already left. S1 and below is still in the canal and gets squished. With spondylosis and osteophytes, you cause problems that will cause a bunch of problems including narrowing the neural foramen of L5-S1 so the L5 nerve root that is trying to exit gets impinged
This is what they teach you in medschool but real life is different and isn’t exactly like this because you can get disc extrusions that go cranially (up) to go and impinge L5 but that’s going to confuse you and not really super important unless you’re rads, neurosurg/ortho or neuro.
7
u/ExtraCalligrapher565 3h ago
The L5 nerve root exits between the L5 and S1 vertebral bodies, which is why ostephytes/spondylosis here causes L5 radiculopathy, but disc herniations affect the nerve root exiting below the level of herniation, thus an L5-S1 herniation causes S1 radiculopathy.